Butt-wink: it’s a rather odd term isn’t it? If you’re reading this, you may have had someone tell you that you have this so called ‘butt-wink.’ Perhaps you’re experiencing some back pain when you squat or when you deadlift and you’re just looking for some answers to why that’s happening.
The butt-wink is a hot topic and it seems to be a never-ending debate in the fitness and medical world on whether it is safe or not. In this article, we would like to explore the mechanism of a butt wink, how to assess it, and discuss what it means for you.
What is A Butt-Wink?
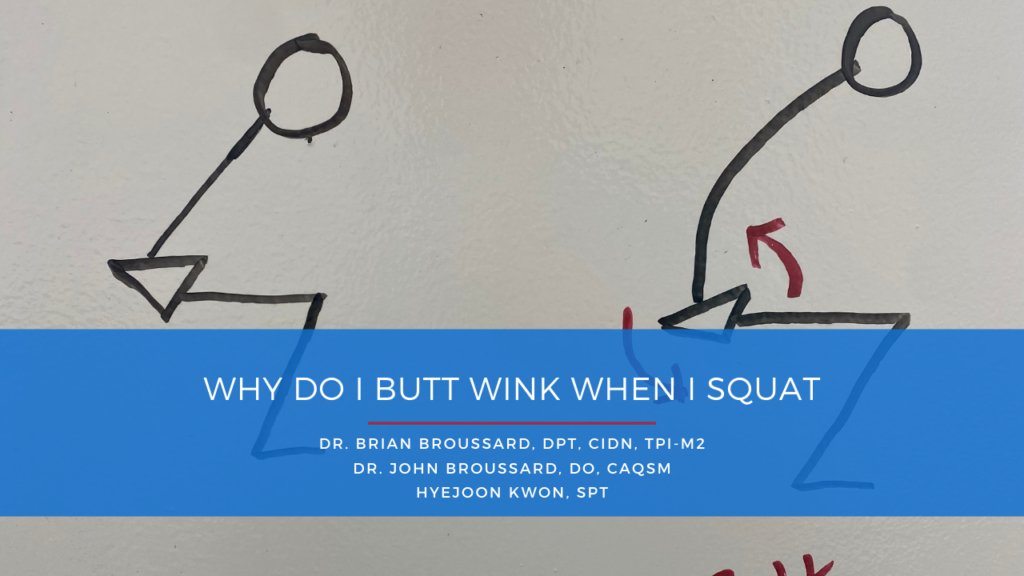
Simply stated, a butt-wink is a posterior tilting of the pelvis (flexion of lumbar spine) that happens either at the bottom or below 90 degrees of the squat.
This movement can be pretty easy to spot when looking at someone’s squat. However, there are times when a butt-wink can appear only when loaded or only unloaded. These variances are important to uncover and analyze for each person because they each tell different stories. We’ll talk about that in a bit.
This excessive lumbar flexion or rounding during the squat will significantly reduce force production capacity at the bottom range of your squat. Simply put, you’re in a sub-optimal position to develop and transmit the force needed to stabilize your spine and perform the lift effectively. Thus, the reason why repetitive movements of flexion and extension under load have been linked to disc herniations and other back injuries.

Recent research on various movement pattens such as the good morning, kettlebell swing, and the squat state that a neutral spine is a ‘range’ and It is not a ‘fixed’ position, meaning, there is some room for movement. So, when we are talking about a squat, a small amount of tilting is unavoidable to a certain degree. Then, the question goes, if it is a range, then how much posterior tilting of the pelvis (“butt wink”) is too much? To find out, it is important to observe the starting position and finishing position, rather than just seeing the motion of pelvic tilt. This is important because you may just get an athlete that likes to start out with more extended lumbar spine at the top then gets into neutral position at the bottom.
Analyzing Mobility
When we’re assessing an athlete, we want to get a global view of the athlete doing functional movements and then we want to break that movement down into individual components. So, we do a pretty comprehensive physical assessment to identify limitations at the ankle joint, hip joint, and the joints in the spine. The spine is most important for the overhead squat variations.
Hip Mobility
Adequate hip flexion, internal rotation and external rotation are all needed to have a full and complete squat. We look to see if the athlete can touch their quads to their abdomen while landing on their back to assess hip flexion. We can assess hip internal rotation (IR) and external rotation (ER) in sitting or we can have the athlete laying on their back with their hip at ninety degrees, while we passively move their leg. We’re looking for 45 degrees of ER and 30 degrees of IR. We can find some variations across the board, but finding limitations reveals which direction needs more of our focus.
Other hip tests we use are the scour test and the quadruped rock back test. The scour test is done by the therapist moving your hip through different ranges of motion, basically hitting all ranges of the joint. This can also be helpful in determining if there is a potential injury within in the joint that we need to focus on. The quadruped rock back test is basically mimicking the squat movement while you are on all fours. This allows us to see if you can coordinate the movement of the pelvis and spine without load.
Ankle Mobility
The next joint that is of prime importance is the ankle joint! Ankle limitations can be from either a mobility issue or a flexibility issue. We assess this by performing a 1/2 kneeling knee to wall test. We place the athlete in 1/2 kneeling with their hips square to the wall. We place our fist between their big toe and wall, then we have the athlete move forward in effort to touch the knee to the wall. One big pitfall here is allowing the knee to drift medially (toward the midline). If the athlete feels restriction in the back of the heel, then it’s likely due to some soleus muscle tightness. If it’s felt in the front of the ankle, then we can attribute that to joint stiffness. It is important to note that all things are always black and white, which is why it is important to get a hands-on assessment with a physical therapist who’s also a movement specialist.
Limited dorsiflexion (DF), either by the joint or soft tissue, will dramatically impact the squat by forcing you to compensate through the hips, spine, and pelvis. The hip tries to make up for the lost motion and when the hip runs of it’s motion, the pelvis and lumbar spine are next in line to compensate – enter butt wink. Although ankle mobility issue can be mitigated by utilizing weightlifting shoes, one must start looking into improving ankle dorsiflexion mobility until they can pass the wall dorsiflexion test for various other health reasons.
Squat Stance/Positioning
First thing we should look at is the anatomical structure of the hip. Because, if an individual has a hip anatomy that does not allow for deeper squat, no amount of mobility drills, form corrections, and stretching will improve their squat.
- Acetabular Anteversion is the term used to describe forward placement of hip sockets. This offers better hip flexion ROI (this makes sense because the socket is more towards forward and hip flexion occurs at the front side of the hip) and retroverted acetabulum (backward placement of hip socket) will limit the flexion ROM by causing femoral neck to contact the acetabulum before achieving desired squat depth, leaving no choice but to roll the entire pelvis backward if forced to continue squatting down. In fact, Retroverted acetabulum has shown to not only decrease hip flexion ROM but also likely increase the risk of femoral neck compression injuries called FAI (where bony ridge of acetabulum presses into the femoral neck and creates irritation)

The Acetabulum structure (hip sockets) on the left faces more forward (and even a bit more superiorly) as we can clearly see the socket from a front view compared to the structure on the right. This structure is suited for greater depth in squat by allowing greater range of hip flexion.
- The depth of hip socket matters also. As guessed, deep hip socket means less ROM in all direction including flexion, but this structure would add more stability in the joint which will make optimal for weight-bearing / impact activities such as running.

We can look at the radiographs above. #1 clearly has deeper hip sockets which will likely be more sturdy and good for producing power at various weight bearing activities, but will wind up creating bone to bone contact much sooner in the bottom range of motion compared to the image on the right, which would have almost no bone to bone contact preventing end range depth.
Thus, if you are born with retroverted acetabulum, thick femoral neck, and deep hip sockets, achieving depth in squat without butt wink would be nearly impossible.
Most of the time, by teaching those individuals their own optimal stance and depth and working on the midline stability at the bottom position, they will be able to exhibit a decent looking squat.
If that worked, awesome, you just need to mimic that stance when you squat and limit the chances of having any impingement issues. If it didn’t work, you could try going even wider, but if that doesn’t work you might have just found your anatomical limit to how much flexion you’re going to get.
Motor Control Work
A butt wink can happen from a mobility limitation or a stability deficit. It’s important to determine which one it is because the path to correcting it looks completely different. If it’s a motor control or stability issue, then we must address this with specific stability work throughout the range of the squat.
Because what good is mobility if you can’t use it effectively.
An example of this is using a counterbalance to squat. This allows them to engage their core more effectively and shift their center of gravity, leading to a more upright posture and reduced chance to butt wink. We can even hold at the bottom position and perform press-outs to work on midline stability and tension.
Before wrapping up, it would be important to mention something about tightness. Unless you have excessive hamstring tightness, the hamstring rarely gets in the way of achieving your max depth potential in a squat. Although it is true that the proximal attachment of the hamstring gets stretched during hip flexion, potentially pulling on the pelvis into posterior pelvic tilt. However, a lot of that tension is dissipated at the hamstring’s distal attachment during knee flexion, making hamstring’s contribution to butt wink somewhat minimal. Usually the main issue lies elsewhere.
These are some of the things that our team at the Alliance Regen & Rehab typically look in our athletes before moving into treatment. Depending on the outcome of the assessments, our treatment approach can vary significantly.
In terms of physical therapy and performance, our Doctors of Physical Therapy don’t treat these problems with just clamshells and hot packs. Our treatments include exercises progressions that resemble the movements you’re trying to get back to. We treat you as an athlete and our goal is to get you to your destination, not leave you 1000 miles away from it with boring and easy band exercises. If we do need to look at the hip with more detail, such as imaging, then we do have a sports medicine physician on-site that can perform a diagnostic ultrasound scan!
If you have hip pain or any other types of restrictions that limit you from performing your best in the gym or the field, we can help maximize your potential and reduce risk for future injury!
It’s going to be finish of mine day, however before ending
I am reading this great article to improve my know-how.
Hello very cool site!! Guy .. Beautiful .. Superb .. I’ll bookmark your site and take the feeds also?
I am happy to search out a lot of helpful info
right here in the submit, we want work out extra techniques in this regard, thanks for sharing.
. . . . .